
This information aims to answer some of the questions you may have about squint surgery. However, it does not cover everything as every patient and squint is different. Your surgeon will discuss your particular case with you. Please ask the clinical staff about anything you want to be made clear. What is the aim of… Continue reading Squint Surgery in Adults
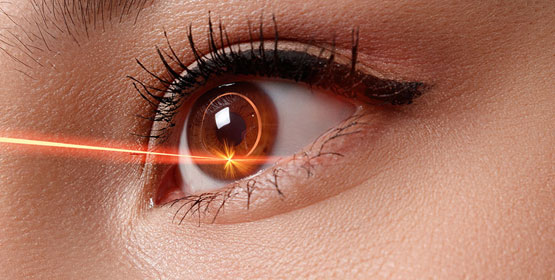
Selective Laser Trabeculoplasty

Selective Laser Trabeculoplasty (SLT) is a procedure used to reduce the pressure in the eye (also known as intra-ocular pressure). A laser beam is applied to the drainage channels, which helps to unclog them. This means the aqeous humour flows through the channels better, reducing the pressure in the eye. This is not a permanent… Continue reading Selective Laser Trabeculoplasty
Refractive Surgery
Most refractive errors can be corrected (or at least improved) by means of Refractive Surgery. This is a generic term, which comprises both Laser Refractive Surgery and correction by means of lens implants inside the eye. The latter is called Phakic intraocular lens (IOL) surgery. Most refractive errors can be corrected (or at least improved)… Continue reading Refractive Surgery
What is Posterior Vitreous Detachment? Causes, Symptoms & Care

PVD is a common degenerative change, which affects one or both eyes in many people after middle age. It may present earlier in shortsighted patients or those who have sustained traumas to the eyes. Thickening of the jelly casts shadows on the retina and are seen as floating shapes. These black “floaters”in your vision move… Continue reading What is Posterior Vitreous Detachment? Causes, Symptoms & Care
Post-Operative Instructions

Following Retinal Surgery on leaving the hospital you are advised to have a quiet evening at home and to avoid strenuous exercise. For General Anaesthetic patients, as above and: Do not drive a vehicle Do not make any crucial financial decision Do not eat heavy meals or drink alcohol for 24 hours after being discharged
Lacrimal Probing in Children

The tear duct is a channel/passage which runs from a tiny opening in the medial lids through the bone to the inside of the nose, and drains the tears and mucus the eye produces. It should open just before or just after birth but sometimes remains blocked for a considerable time after that, causing watering… Continue reading Lacrimal Probing in Children
Types of Diabetic Retinopathy

Introduction Diabetic retinopathy is a complication of diabetes and leads to high blood sugar, resulting in retinal disease, which can interfere with its ability to transmit images to the brain through the optic nerve. Blood vessels in the retina play an important role in supplying it with oxygen and nutrients, which keep it healthy and… Continue reading Types of Diabetic Retinopathy
Dacryocystorhinostomy
[:en]Blocked Tear Duct. The tear ducts start at the inner corner of the eye with two small holes in the corner of the eyelids. Each hole is known as a punctum, they lead into small tubes known as canaliculi, which in turn drains into the lacrinal sac. This lies between the corner of your eye… Continue reading Dacryocystorhinostomy
Amblyopia Therapy

What is Amblyopia? Lazy eye – the medical term is Amblyopia – is a common eye condition amongst younger children. It means that one eye is not developing properly and becomes ‘lazy’ because the brain is working harder with the good eye to compensate. The problem is that if the brain ignores the lazy eye,… Continue reading Amblyopia Therapy
Ophthalmologist
[:en]Patients who need further specialist treatments for their eyes go to an Ophthalmologist. An Ophthalmologist is a medical doctor who specialises in the medical and surgical care of the eyes, visual system and in the prevention of eye diseases and injuries. They provide the full range of care including routine eye examinations, diagnosis and treatment… Continue reading Ophthalmologist
Orthoptist
[:en]Children who need to see an eye Specialist will initially go for a review with an Orthoptist – a health professional who specialises in eye movement problems and disorders that affect how the eyes work together. These conditions are typically diagnosed in childhood; so Orthoptists are highly experienced in examining children of all ages and… Continue reading Orthoptist
Optometrist
[:en]Patients who need to have a vision test or have glasses/contact lenses fitted to correct their vision, go to an Optometrist. An Optometrist is a health care professional who is licensed to provide primary eye care services. Optometrists examine and diagnose vision defects such as near sightedness, farsightedness, astigmatism (blurred vision), and presbyopia (reduced ability… Continue reading Optometrist