
Diabetes is a significant public health issue across the Gulf region, including the UAE, Saudi Arabia and Kuwait. According to the international diabetes federation, approximately 20.7% of UAE adults are living with diabetes, equating to around 1.25 million adults, or 1 in 6 adults. Diabetes is a chronic condition that affects how the body absorbs,… Continue reading What is Diabetic Retinopathy
What is Keratoconus?
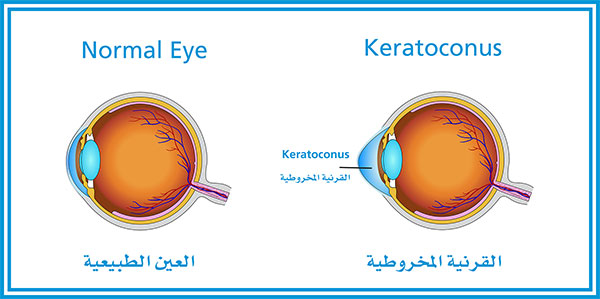
This blog on Keratoconus has been contributed by Dr Osama Giledi, Consultant Ophthalmologist, Specialist in Cataract, Cornea and Refractive Vision Correction Surgery What is Keratoconus? The word Keratoconus comes from two Greek words: kerato (cornea) and konos (cone). Keratoconus is a degenerative disorder of the eye in which the shape of the cornea, which is… Continue reading What is Keratoconus?
Teaching session for Al Jaber Optometrists in October, 2017
[:en] [:ar] [:]
Teaching session for Al Jaber Optometrists in October, 2017
[:en] [:ar] [:]
Teaching session at a hospital in Mainland China in November & December 2017
[:en] [:ar] [:]
Teaching session for School Teachers and Nurses in November, 2017.
[:en] [:ar] [:]
What is Uveitis?

This week’s blog on Uveitis has been contributed by Dr Avinash Gurbaxani, Consultant Ophthalmic Surgeon in Uveitis and Medical Retinal Diseases and Cataract Surgery. Uveitis is not a single disease but a clinical spectrum of symptoms and signs caused by a variety of medical conditions. Although it accounts for about 1% of all eye diseases, Uveitis… Continue reading What is Uveitis?